This module discusses casualty preparation for evacuation during the Tactical Field Care (TFC) setting.
All
Service Member and Combat Lifesaver training educates non-medical
personnel about supporting the casualty evacuation preparation process.
As a Combat Medic you will supervise that preparation process and be
responsible for the transition of care from the Tactical Field Care
setting to the Tactical Evacuation Care (TEC) phase.
There are eight cognitive and one performance enabling learning objectives in this module.
While
focusing on identification of the important principles of preparing and
staging casualties for evacuation you will also be learning about
several related topics, to include the importance of pre-mission
training, considerations for evacuation of a casualty with a suspected
spinal injury, litter and evacuation equipment selection, and
considerations for evacuation of ambulatory casualties. Additionally,
the process of transitioning care to evacuation personnel and the
responsibilities of tactical force personnel during the evacuation
process will be discussed.
Afterward, you will demonstrate the preparation of a casualty for evacuation in the Tactical Field Care phase.
Proper
preparation for evacuation will help to ensure a smooth handover to
evacuation personnel. Keep in mind that the transition is challenging
for several reasons. The tactical environment may be somewhat insecure,
the environment may involve loud noise conditions (like under spinning
helicopter rotor blades or at the tail of a fixed-wing evacuation
aircraft), and the receiving asset may be moving slightly (like on small
boats rocking back and forth in rough seas). A smooth transfer of care
in these hectic environments is facilitated by well-prepared casualties,
preplanned procedures, rehearsals, and effective communication.
Although
every tactical situation and set of casualties will dictate the way you
prepare casualties for evacuation, there are some basic principles
common to all of them that can guide your actions and ensure the best
possible outcome for the casualty.
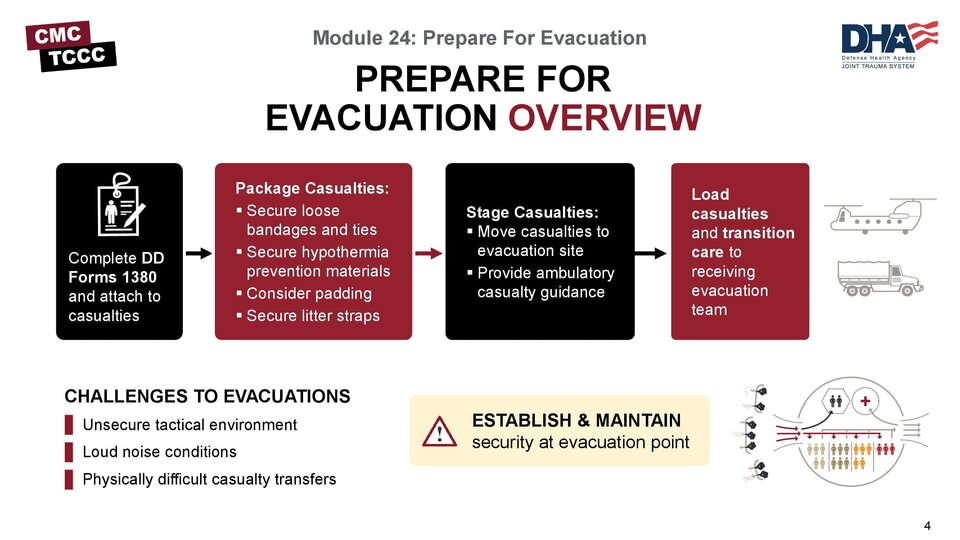
In most situations, the first
thing you will do is prepare each casualty for evacuation. Some of the
steps and individual tasks may be delayed until the staging phase, if
the tactical situation mandates casualty movement prior to completion of
preparation for every casualty, but usually the preparation is
integrated into the last steps in the tactical trauma assessment and can
be accomplished prior to movement. This is when many of the steps in
the TCCC Guidelines are executed, to include securing the DD Form 1380,
the loose ends of wraps, bandages, and hypothermia prevention materials,
and tightening litter straps prior to movement.
Once the
casualties are prepared, the next step is to stage them for evacuation.
This might be done twice, once near the treatment area and again at the
evacuation location, if the evacuation pick-up site is located at a
distance from the treatment site and there is a delay in evacuation.
This is also the time when instructions will be provided to casualties,
in particular the ambulatory casualties, to reduce the workload on the
evacuation team during the casualty pick-up process.
When the
evacuation assets are approaching, it is vital to secure the evacuation
zone using the tactical forces personnel provided to you by the local
unit leadership.
And lastly, when the assets arrive, the
casualties must be properly loaded, following the guidance of the
incoming evacuation personnel. As a Combat Medic, you will be
responsible for the transition of care from your team in Tactical Field
Care to the receiving evacuation team as the casualty enters the
Tactical Evacuation Care phase.
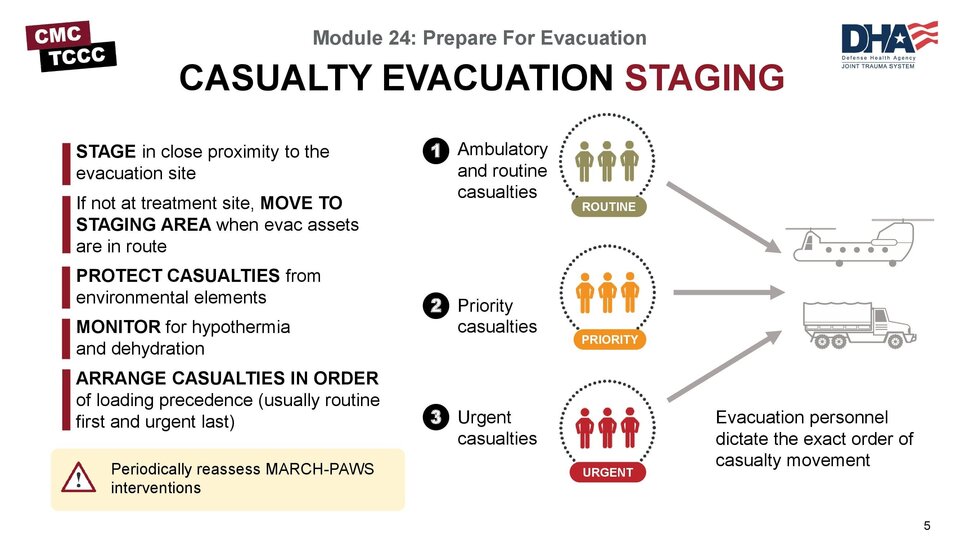
Staging
typically occurs in close proximity to the evacuation site, and if not
co-located with the treatment site, the casualties are moved there in
advance. Although you do not want to have the asset waiting for the
arrival of the casualties, you also do not want to have the casualties
arrive too soon if the environment is not ideal for waiting long periods
of time.
Remember, when moving casualties over long distances,
tourniquets, dressings, IV lines, or other interventions should be
checked periodically to ensure they are intact and functioning. You
should definitely do this upon arrival at the staging site, if not along
the way.
In transit and once at the staging area, casualties
should be protected as much as possible from environmental elements
(like the sun, rain, wind, or cold) and observed for signs of
hypothermia or dehydration.
At the site, the casualties should be
arranged so that they can be loaded in sequence, according to their
movement priority and clinical status. This may be dictated by unit
procedures, or it may be provided by the evacuation platform personnel.
In general, when feasible, ambulatory and routine casualties are loaded
first, followed by priority casualties, and urgent casualties are loaded
last. This allows for urgent casualties to have the least amount of
time on the evacuation platform, and more importantly, to be the first
off of the asset once it arrives at its destination.
Once the
evacuation asset arrives, the personnel responsible for loading
casualties will dictate the order of casualty movement, regardless of
the way the casualties were arranged by the ground medical team.
As
you can imagine, several members of the unit are involved in
choreographing a successful casualty evacuation. If the first time that
unit members are involved in this process is during an actual
evacuation, there is a significant risk that the team will not function
well and the evacuation process will be delayed or the transition of
care will be less than optimal, which could result in an adverse
clinical outcome. So, it is important that pre-mission rehearsals be
part of every unit’s training, both at home station and down-range.
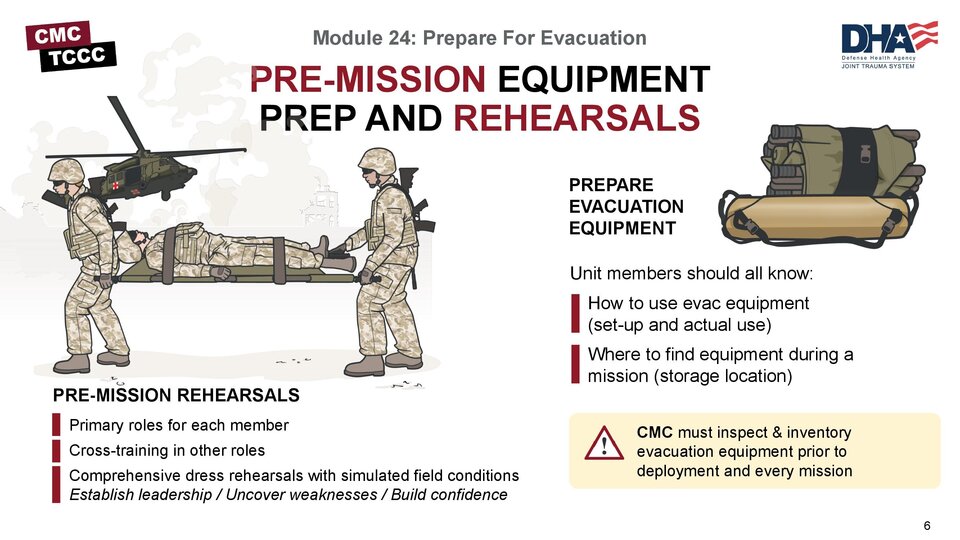
These
rehearsals not only involve understanding the primary role each unit
member will be expected to perform, but cross-training unit members so
that they can assume the duties of one of the other members, should that
member become a casualty and need to be replaced. It is not enough to
talk through the process, it is essential to run dress rehearsals where
unit members perform their functions under your supervision. Carrying
out the individual tasks uncovers problems that can be easily resolved,
and builds confidence in your unit personnel.
Another part of the
pre-mission process is preparing evacuation equipment. At the onset of a
deployment, most equipment is usually stocked and functional; but that
should still be confirmed prior to departure from home station and after
arrival. Once deployed, not only do you need to ensure equipment is in
working order, you need to ensure all required equipment is present, as
prior missions may have used assets that were not properly resupplied.
This emphasizes why it is important to ask for equipment replacement
during the evacuation request process. Also, key members of the unit
need to know where the equipment will be located when out on a mission,
and how to access it, as you will not have time to search for the
equipment when you are providing or supervising casualty treatment.
Understanding
that each situation is unique, there are some basic measures that
should be followed for all evacuation preparation scenarios. The TCCC
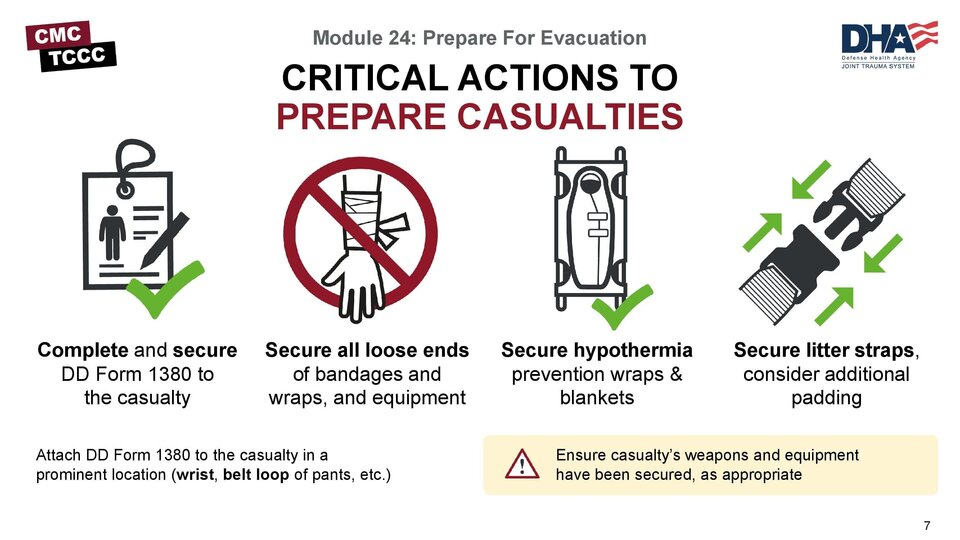
Guidelines outline the critical actions that should be followed.
Although usually handled by unit leadership and fellow team members,
ensure casualty’s weapons and equipment are secured, as appropriate.
Complete
and secure the DD Form 1380 to the casualty. Some hypothermia shells or
patient transport covers have a transparent pouch where you can put the
DD Form 1380, but many do not. Options for securing it to the patient
include attaching it to their wrist or other body parts if there is a
band or taping it to them or their packing materials. Remember that the
goal is to not have the casualty and their DD Form 1380 separated as
they go through their continuum of care. So, however you secure it, make
sure it will stay with the casualty.
Secure all loose ends of
bandages and wraps. Loose treatment interventions pose risks for the
casualty, the responders, and even the evacuation assets. For the
casualty, a loose wrap or exposed tourniquet windlass can be caught on
individuals working around the casualty or on the evacuation platform
and be compromised, requiring that the intervention be reassessed and
treated again, potentially worsening the clinical situation or delaying
evacuation. Responders and personnel working around the casualty can get
caught by loose interventions and hurt themselves, for example by
tripping over the loose wraps. And anything that isn’t secure has the
potential for breaking loose and can fly free, particularly in rotor
wash or at the tail of an aircraft, both creating a projectile that can
hurt personnel and debris that can damage the evacuation asset.
Secure
hypothermia prevention wraps, blankets, and straps. Similar to the
prior discussion, the actual casualty wraps can be a problem for the
very same reason. But even if they don’t break free and create those
problems, if they are not properly secured the hypothermia prevention
measures will not be effective. The wraps need to retain any heat being
produced by the casualty or their heating device, which won’t happen if
they are loose.
Secure litter straps as required. Consider
additional padding for long evacuations. Litter straps are commonly
loosened to allow access to the casualty for reassessment purposes, and
occasionally they are not re-tightened afterward, either for easy access
or casualty comfort. However, when transporting the casualty and while
in the evacuation asset, this can be a significant safety hazard. Be
sure to check all straps, and ensure each casualty has at least two
straps. Litters are, by their very nature, uncomfortable. For short
periods this is usually tolerated fairly well. But for prolonged waiting
periods and long evacuation, this can add to casualty pain and stress
and adversely affect their outcome. Whenever possible, add padding to
provide casualty comfort, even if the casualty is not complaining of
being uncomfortable.
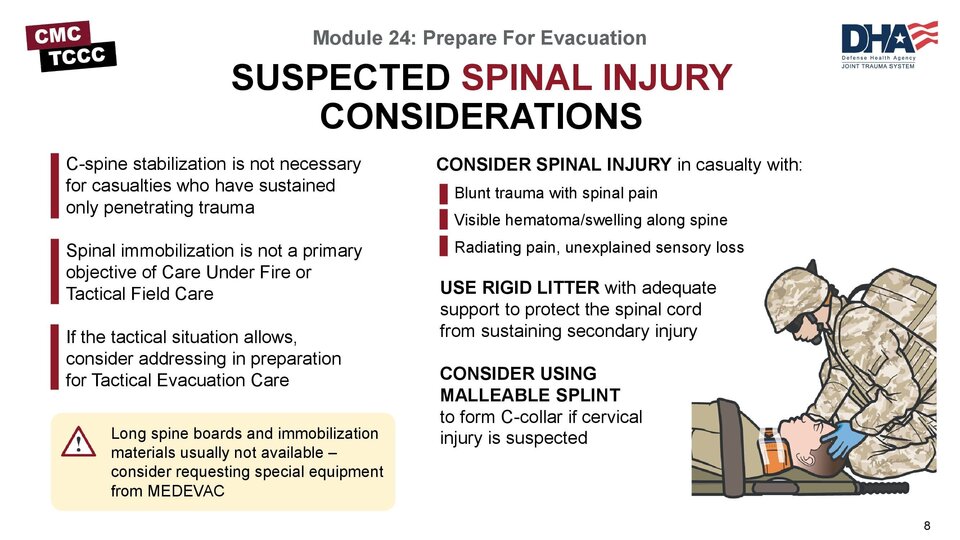
The
TCCC Guidelines highlight that cervical spine stabilization is not
necessary for casualties who have sustained only penetrating trauma.
Several studies and guideline papers from professional societies mirror
that guidance. And because of the tactical considerations and treatment
priorities in the battlefield environment, spinal immobilization, as a
rule, is not a primary objective of Care Under Fire or Tactical Field
Care phases.
However, as the casualty transitions from TFC to
TEC, there may be time and a permissive environment to address suspected
spinal injuries. If the casualty is a victim of blunt trauma and
experiencing spinal pain, has visible swelling or hematomas along the
spine, or is experiencing radiating pain or unexplained loss of
sensation in their extremities, spinal injury may be suspected.
If
suspected, a rigid litter that provides adequate support to help
protect the spinal cord from sustaining secondary injury should be used,
if at all possible. Long spinal boards and classic spinal
immobilization materials are usually not available. If appropriate, they
can be requested when calling in the 9-Line. If the injury involves the
C-spine, a cervical collar can be improvised from a malleable splint or
other material and applied to the casualty before moving. But if the
suspected injury is at a lower level, the rigid litter with firmly
applied straps to prevent undesirable movement during casualty transport
should be adequate.
During the transition of care to the
receiving evacuation team, the suspicion of a spinal injury and any
measures you have taken should be communicated.
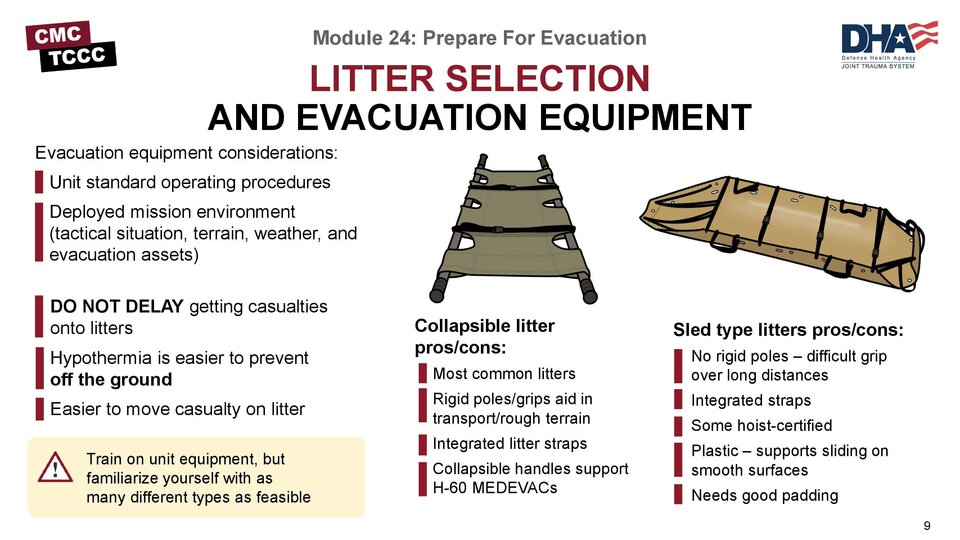
The
types of litters and evacuation equipment you have access to will be
determined by a combination of your unit standard operating procedures
and the deployed mission environment. Ideally, you will have access to a
few different assets, as each of them has advantages and disadvantages
based on the tactical environment (terrain, weather, hostile threats)
and the evacuation assets (air ambulance, air asset of opportunity,
ground vehicles).
Evacuation equipment (like litters &
packaging materials) should be prepared by other unit personnel while
treatment is rendered by medical personnel. Do not delay getting
casualties onto litters as it is easier to prevent hypothermia when
casualties are off the ground and casualty movement is facilitated by
being on a litter.
Train on the equipment your unit supplies, but
make every effort to expose yourself to, and even train on, other types
of equipment, as you may very well encounter them when deployed. It is
definitely an advantage to have equipment familiarity prior to using
them in an operational setting.
The quad-fold Talon II® litter is
perhaps the most common litter currently being used. Once set up
properly, it has rigid poles, and the grips help make it advantageous
for transporting a casualty in rough terrain. It has integrated litter
straps and the mesh material makes it easy to clean and useful in
decontamination scenarios. Also, the Talon II litter has collapsible
handles and will fit into standard H-60 MEDEVAC platforms, whereas some
of the other litters like the Raven 90C® bi-fold litter do not fit
properly.
Skedco™ litters are commonly used tactical litters in
light infantry and airborne units. They do not have rigid poles, so
carrying them by their handles is not easy and can be tiresome over
distances. However, they do function well as drag or slide devices, and
if the terrain is smooth, they can be easily pulled by one or two
responders, being cautious not to let them slide out of control when
going downhill. They are often used to carry gear and ammunition into
the mission and carry casualties out. And properly rigged, they can be
hoisted into a helicopter or Osprey, although not all versions are
hoist-certified.
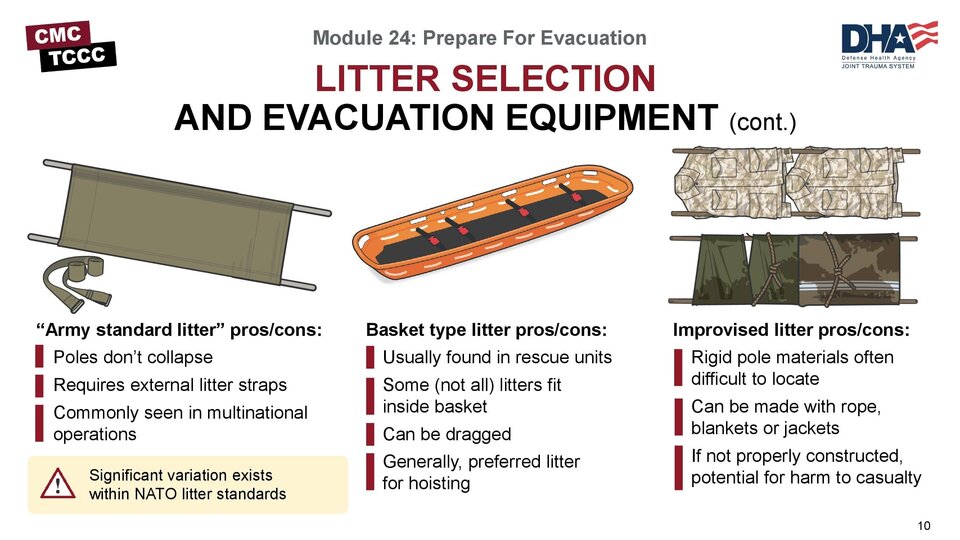
The
“Army standard litter” is another option for a tactical litter. It does
not have preinstalled litter straps, so these will need to be carried
on the mission as well. Many countries have variations of this litter,
with rigid poles and canvas material liners, so it is common to see
these in multinational operations. There is wide variability in what is
considered NATO-standard, and not all NATO-standard litters will fit
into US evacuation assets.
The Stokes litter may be used by
rescue units but is not typically carried by ground combat units. It is a
basket litter, sometimes made of wire mesh and metal materials, and
sometimes plastic. The casualty can usually be placed inside the basket
in a Skedco litter, but it will not accommodate a rigid pole litter and
might require casualties be transferred if the evacuation platform
requires the use of this litter. Stokes litters can be dragged by two
rescuers, if necessary, but can also be carried by four.
In the
absence of a dedicated litter, it is possible to fashion improvised
litters. There are several techniques, but most involve selecting rigid
pole-like materials and then using ponchos, poncho liners, blankets,
field jackets, or other field-expedient materials to form the bed of the
litter. A rigid transport platform, like a door, is also an option if
properly padded. Casualty safety is important, so care must be used to
ensure any improvised litter will be able to support the casualty’s
weight, be relatively easily carried by a litter team, and not risk
significant casualty movement during transport.
Choosing a litter
may be based solely on equipment availability; but if multiple options
are available, then base your decision on a combination of the terrain
and tactical considerations, the unit personnel you have to support
casualty movement, and the evacuation asset you anticipate using.
The
TCCC Guidelines highlight the requirement to provide instructions to
ambulatory patients as needed. As part of the casualty preparation phase
or the evacuation staging phase, depending on the situation, time
should be taken to address ambulatory casualties and how they will be
handled during the evacuation process.
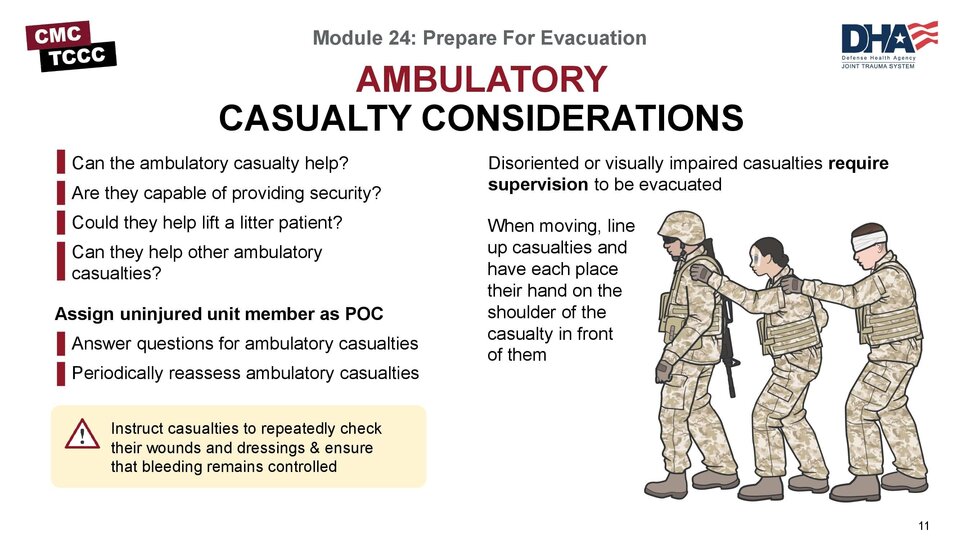
Once you have determined
that a patient is able to ambulate, it is important to assess their
capabilities to assist in the evacuation process, either through being
self-sufficient or perhaps even supporting others. For example, are they
capable of providing security? Could they help lift a littered patient?
Or can they help watch out for and/or care for other ambulatory
casualties?
If they are able to help with the evacuation process,
provide them clear guidance on the role you want them to perform and
assign an uninjured unit member to be their point-of-contact (POC) if
the casualty feels their situation is changing and they can no longer
help out. Have that POC keep an eye on them, too, as they should be
reassessed for potential changes in mental status or capabilities from
time to time.
Disoriented or visually impaired casualties require
supervision to be evacuated, even as ambulatory casualties. This can be
done by a non-medic and done in groups if there are several. When they
need to move as a group, like when approaching the evacuation platform,
they should line up and each place their hand on the shoulder of the
casualty in front of them and follow their lead, with the lead casualty
being someone without visual impairment or disorientation (another
casualty, a Combat Lifesaver or other uninjured non-medic).
To
reduce the workload on the supporting medical personnel, instruct
ambulatory casualties on repeatedly checking their own wounds and
dressings to ensure that bleeding remains controlled and there isn’t a
change in their status, advising them about who to notify if there is a
change.
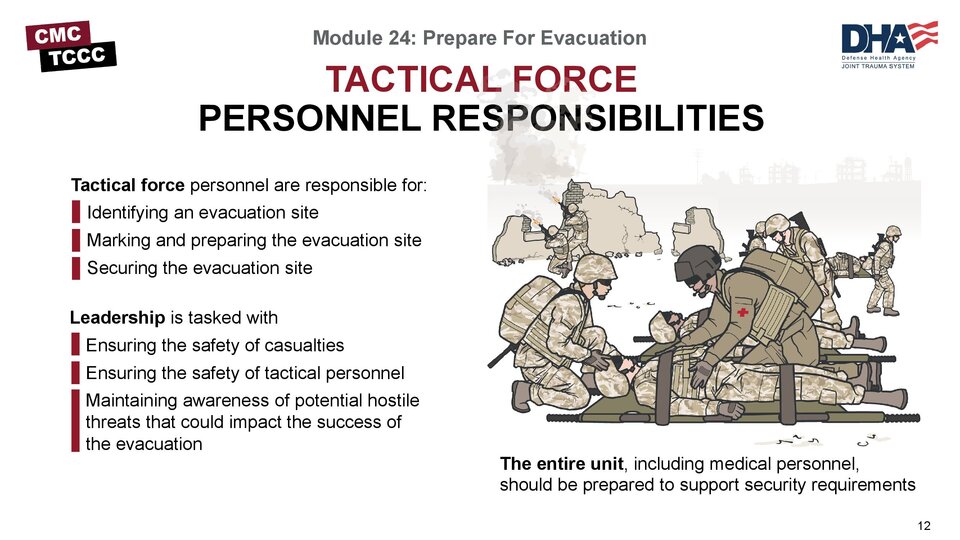
Tactical
force personnel are responsible for identifying, securing, marking, and
preparing the evacuation site (helicopter landing zone, ambulance
loading point, etc.) in advance of the arrival of evacuation assets.
Unit
standard operating procedures will likely govern security at the
evacuation point, and the entire unit, including medical personnel,
should be prepared to support unit leadership in that process. The
potential for exposing the unit and the evacuation team to hostile
forces is significant and maintaining security is vital to the success
of the evacuation process.
Tactical leadership will define the
security measures and inform medical personnel of the parameters that
will guide their casualty staging plan. Throughout the process,
leadership is multi-tasked with ensuring the safety of both casualties
and the tactical personnel who are moving the casualties and maintaining
awareness of potential hostile threats that could impact the success of
the evacuation.
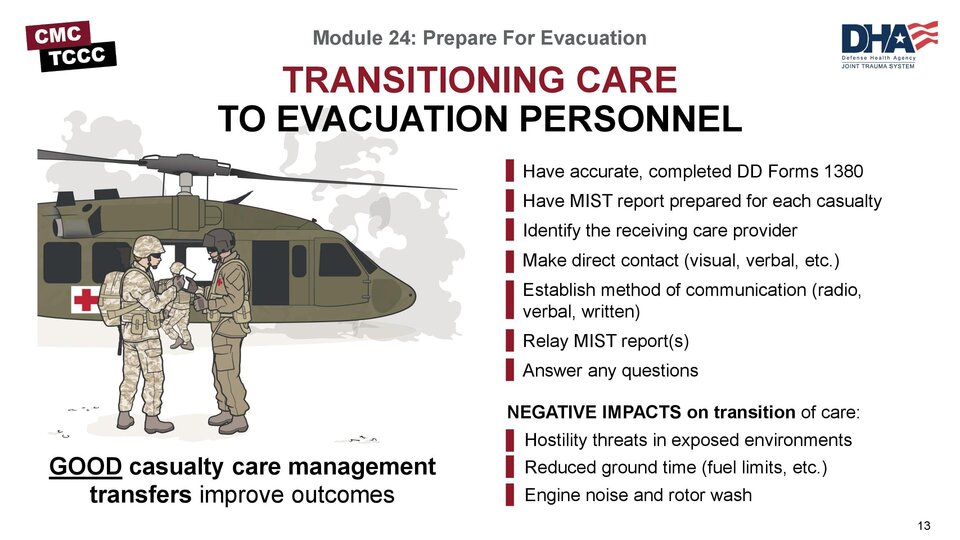
A
critical step in casualty management is successfully transitioning care
from one provider to another. In the civilian setting, there is
overwhelming evidence that less-than-ideal hand-offs and inadequate
communication of patient information lead to poor clinical outcomes.
Despite the fact that there are fewer military-based studies, anecdotal
evidence from battlefield casualty care management transfers indicates
that this is true in the tactical environment, as well.
There are
several environmental factors that can negatively impact the transition
of care and sharing of information in the tactical environment. The
threat of hostilities in an exposed location leads to a requirement to
minimize the time on ground during an evacuation by air assets, as does
the fact that fuel levels may be limited. The noise and rotor or engine
wash can reduce eye contact and hearing thresholds, leading both parties
to look for abbreviated means of communication. The casualty evacuation
process is not part of the unit’s mission objectives and there is
pressure to transition back to normal operations as soon as possible.
All of these things, and more, can have a negative impact on the
transition of care if not mitigated properly.
One very important
tool to help provide adequate casualty information is the make sure that
the DD Form 1380 is fully completed, up-to-the-minute, and accompanies
the casualty throughout their journey.
That said, there are
subtle findings and experiences from assessing and treating the casualty
that are more appropriately passed along in a verbal transition of
care. So, you should be prepared to provide a MIST (Mechanism, Injuries,
Signs, Treatment) report, focusing on those aspects that might not be
self-evident from the DD Form 1380, including your sense of the
casualty’s stability for evacuation.
As mentioned, there are
several factors that might be obstacles to this in the tactical
situation, and you should be prepared to address those as they arise.
Some potential ways to do that include:
Identifying the receiving care provider on the evacuation.
Establishing
direct contact with that provider – through eye, verbal or hand
contact, let them know that you will be providing them information on
the casualties.
Establishing a means of communication – this
might be through direct verbal exchanges, radio communications if they
have a spare headset available, or in worst-case scenarios through hand
motions and pointing at written documentation.
Providing the MIST report, to include treatments that should be continued during the evacuation phase.
Answering any questions that they have prior to departure.
This video will review the basic steps a Combat Medic should follow when preparing a casualty for evacuation.
PREPARE FOR EVACUATION VIDEO
During this module, we went over the key concepts you will need to know to prepare casualties for evacuation.
In
addition to having an overview of the process of preparing and staging
casualties for evacuation, we talked about several areas in more depth,
to include: the importance of pre-mission training, litter and
evacuation equipment selection, critical actions in preparing
casualties, considerations for evacuation of a casualty with a suspected
spinal injury, and considerations for evacuation of ambulatory
casualties. Additionally, the process of staging casualties, the
responsibilities of tactical force personnel during the evacuation
process, and effective transition of care to evacuation personnel were
discussed.
And in the end, you demonstrated the preparation of a casualty for evacuation in the Tactical Field Care phase.
To close out this module, check your learning with the questions below (answers under the image).
Check on learning
Answers
Why is it important to perform pre-mission rehearsals of preparation for evacuation?
If
the first time that unit members are involved in this process is during
an actual evacuation, there is a significant risk that the team will
not function well and the evacuation process will be delayed or the
transition of care will be less than optimal, which could result in an
adverse clinical outcome. These rehearsals not only involve
understanding the primary role each participant will be expected to
perform, but cross-training unit members so that they can assume the
duties of one of the other members.
What goes into selecting a litter?
Choosing
a litter may be based solely on equipment availability; but if multiple
options are available, then base your decision on a combination of the
terrain and tactical considerations, the unit personnel you have to
support casualty movement, and the evacuation asset you anticipate
using.
Name three critical actions in preparing a casualty for evacuation.
Complete and secure the DD Form 1380 to the casualty.
Secure litter straps as required, consider additional padding for long evacuations.
Provide instructions to ambulatory patients as needed.
How should you arrange casualties when staging them at the evacuation site?
At
the site, the casualties should be arranged so that they can be loaded
in sequence, according to their movement priority and clinical status.
This may be dictated by unit procedures, or it may be provided by the
evacuation platform personnel. In general, when feasible, ambulatory and
routine patients are loaded first, followed by priority casualties, and
urgent casualties are loaded last.